Fat embolism after acupuncture – The BMAS Blog
Stimulated by Xu et al 2023.[1]
SvN – silver needle
SSN – stainless steel needle
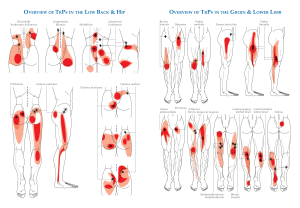
LBP – low back pain
PID – prolapsed intervertebral disc
FFA – free fatty acid
CRP – C-reactive proteinkey to acronyms
This paper popped up on PubMed last night, whilst I was on my way back to London after a weekend of teaching at BMAS House. I had inadvertently deleted my ‘Recent’ folder of references on Zotero, so I went straight to PubMed to see the latest search results with acup* in the title. This paper came top of the list, and I was immediately intrigued as I had never heard of non-traumatic pulmonary fat embolism before, and certainly not following acupuncture.
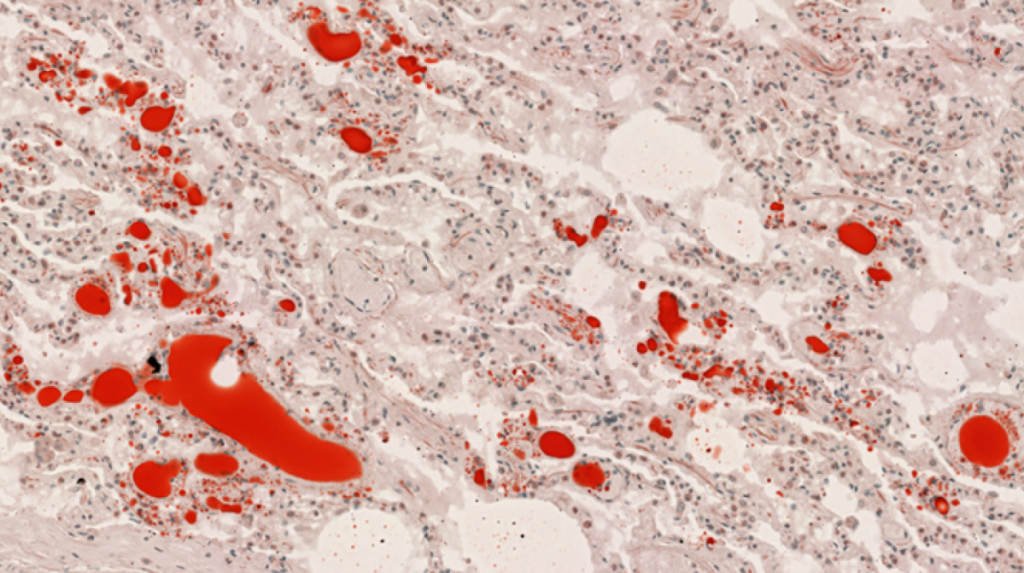
The case is of a 72-year-old woman who experienced dizziness and fatigue immediately after silver needle (SvN) acupuncture. She was assessed in hospital but deteriorated rapidly and died 2 hours later.
I imagine you are wondering about the silver needles. Well, the paper states that the needles used were 1.1mm in diameter, and that there were 30 puncture marks on the skin of the lower back. It was also noted that the skin of the lower back had swelled and that multiple pinholes were oozing blood when the patient was assessed and still alive. Despite all of this, the autopsy report did not consider that needle trauma was sufficient to explain the fat embolism.
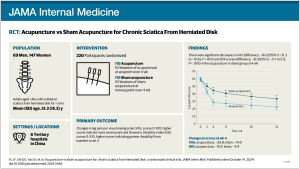
I looked up SvN therapy and found a trial protocol that explained the use of gold and silver needles. Apparently, these metals conduct heat more readily than stainless steel.[2] I was mildly curious about the results of this trial of SvN warm acupuncture versus SSN warm acupuncture in acute LBP due to lumbar PID. It was a moderately sized trial (n=159) but the only difference between the groups was the metal in the needles and the temperature achieved at the skin level (43ºC vs 40ºC).[3]
The SvN warm needle treatment (3 sessions a week for 3 weeks) proved to be significantly superior after the treatment course (week 4) and at follow up (week 16 and 28). This is a very good result; indeed, it verges on being too good, considering that much larger trials of acupuncture in LBP have not been able to differentiate between real and sham needling. I am also curious as to why the published protocol is not referenced in the final report of this trial.
I should note that the needles used in this trial were a mere 0.40mm in diameter as opposed to the 1.1mm ones used in the unfortunate woman in the fatal case report.
Whilst to us acupuncture practitioners in the West, the needling seemed rather traumatic and indeed looked quite traumatic at autopsy, it was not considered traumatic enough to explain the fatal fat embolism. So, what is the mechanism for fat embolism? There are 2 contenders: the mechanical theory and the biochemical theory.[4] I remember the mechanical theory that fat from the marrow at a fracture site can enter broken veins and travel in the circulation to the lungs. It seems straightforward, but I am reminded that it is still a theory.
I had not come across the biochemical theory, which suggests that under stress and the release of catecholamines, FFAs and CRP increase, leading to increased vascular permeability and inhibition of pulmonary surfactants. It is not clear what sequence of events leads to circulating fat globules combining to form globs of sufficient size to block small pulmonary vessels.
I am left wondering whether in this case the acupuncture with 1.1mm needles was stressful enough to tip this individual into forming fat emboli through biochemical means or whether the needling itself was mechanically traumatic enough to start off the process. The forensic pathologist calculated the surface area of contact with the needles and determined that this was insufficient when compared with the required area of blunt soft tissue trauma to cause fat embolism. But this does not consider the enormous pressure generated at the tips of such unyielding needles.
Either way, whilst this is a very interesting case, I think we are probably ok to continue as usual with our 0.25mm or even 0.35mm diameter needles in patients who are relatively comfortable with the stimulus intensity.
References
1 Xu L, Tan X, Chen X, et al. Rare, fatal pulmonary fat embolism after acupuncture therapy: A case report and literature review. Forensic Sci Int 2023;345:111619. doi:10.1016/j.forsciint.2023.111619
2 Li T, Wang S, Zhang S, et al. Evaluation of clinical efficacy of silver-needle warm acupuncture in treating adults with acute low back pain due to lumbosacral disc herniation: study protocol for a randomized controlled trial. Trials 2019;20:470. doi:10.1186/s13063-019-3566-2
3 Li T, Wang S, Cheng K, et al. Comparing the efficacy of two different temperature stimulation in warm acupuncture on acute low back pain: A randomized controlled trial. Integr Med Res 2022;11:100748. doi:10.1016/j.imr.2021.100748
4 Meng Y, Zhang M, Ling H, et al. Nontraumatic Multiple-Organ Fat Embolism: An Autopsy Case and Review of Literature. Am J Forensic Med Pathol 2020;41:131–4. doi:10.1097/PAF.0000000000000544
Published by
Published